Adenomyosis and Fertility: What You Need to Know
For many women, the journey to an adenomyosis diagnosis begins long before they ever hear the word itself.

Free Thursday Consultation
Book Your AppointmentOver the years, I’ve met countless patients who have lived with heavy periods, severe menstrual pain, pelvic discomfort, or unexplained fertility challenges for years. Many have been told that painful periods are simply something they need to tolerate. Others have assumed that their symptoms are a normal part of being a woman because they’ve experienced them for so long.
When these patients finally receive a diagnosis of adenomyosis, their reaction is often the same: relief that their symptoms have a name, mixed with frustration that it took so long to get answers. Part of the challenge is that adenomyosis is frequently mistaken for other conditions. Its symptoms can overlap with endometriosis, fibroids, and what many women dismiss as “just bad periods.” Because of this overlap, the condition can remain unrecognized for years.
If you’ve recently been diagnosed with adenomyosis, or suspect it may be contributing to your symptoms or fertility concerns, this guide will help you understand what the condition is, how it affects reproductive health, and what treatment options may be available.
What is Adenomyosis?
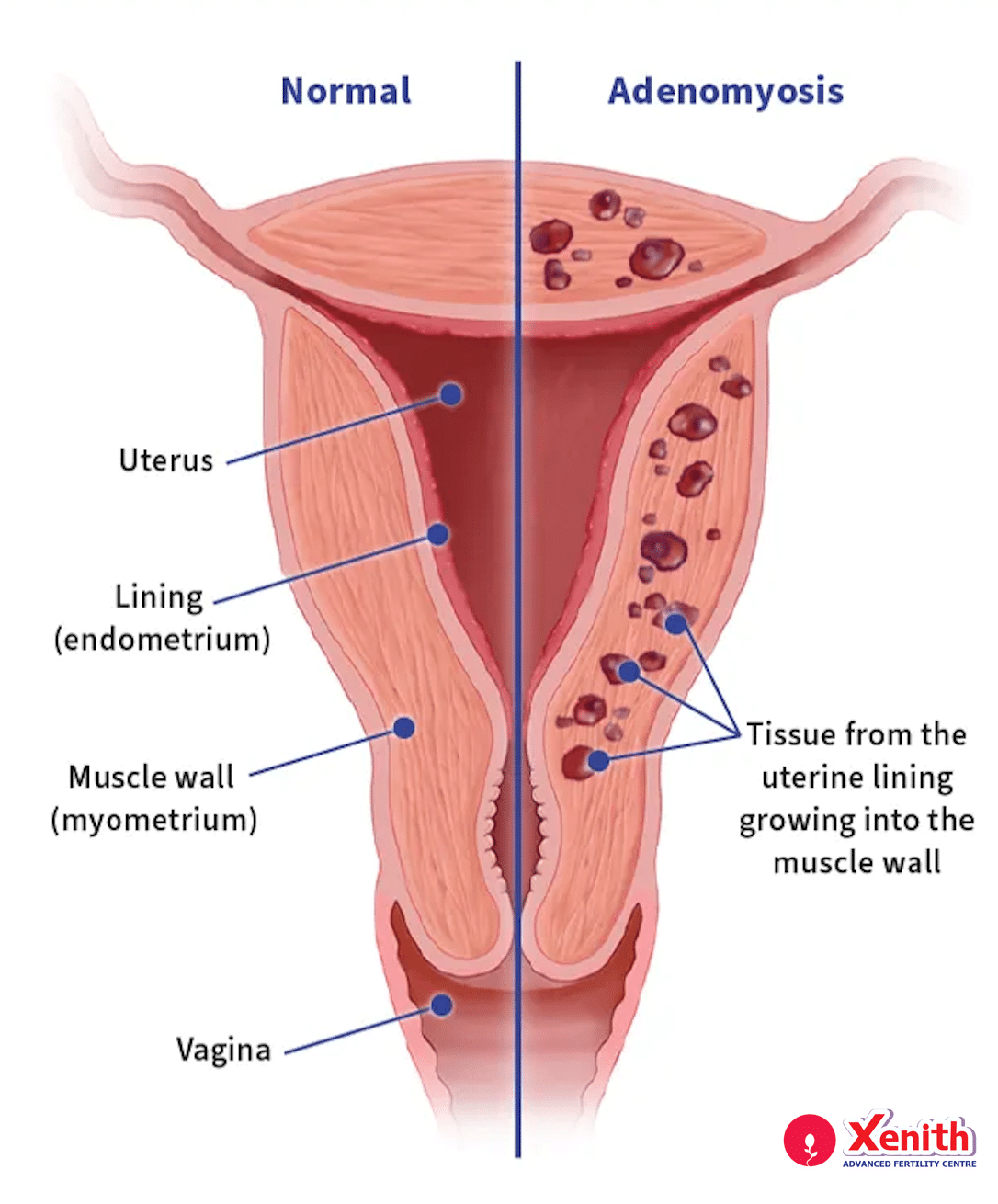
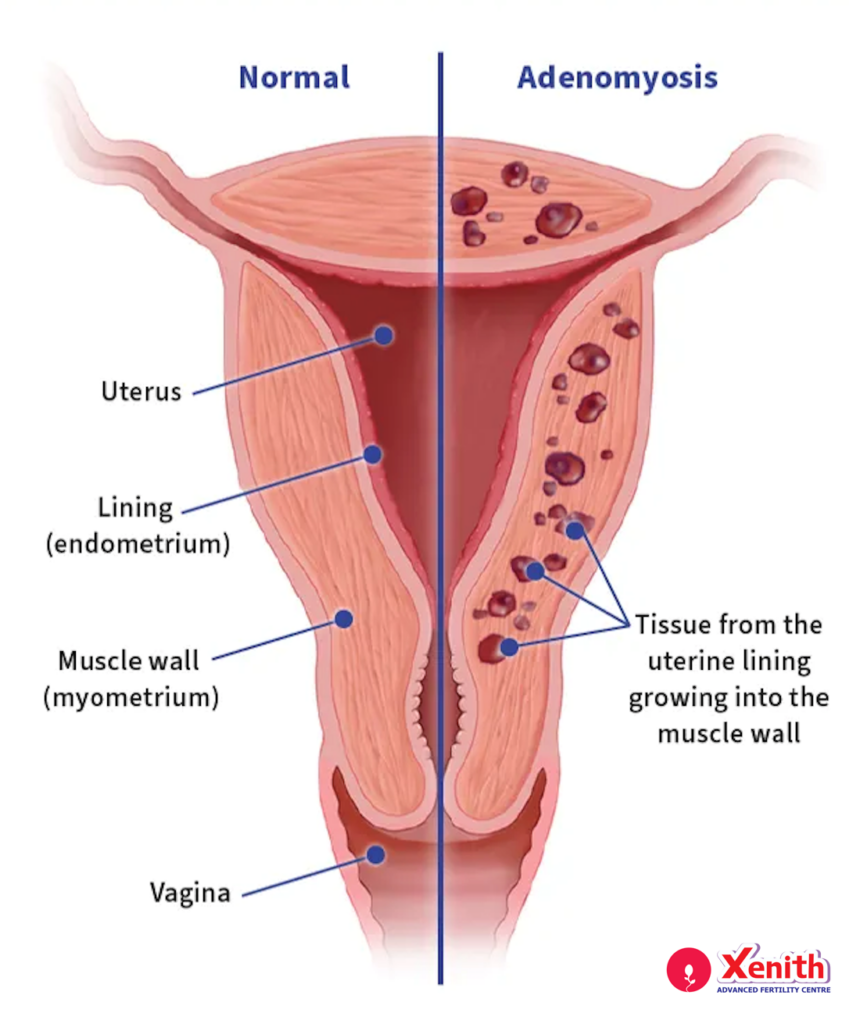
Adenomyosis is a condition in which tissue similar to the lining of the uterus, known as the endometrium, grows into the muscular wall of the uterus itself.
To understand why this matters, it helps to think about how the uterus is structured. Normally, the endometrial lining sits inside the uterine cavity and thickens each month in preparation for pregnancy. In adenomyosis, endometrial tissue becomes embedded within the muscle layer of the uterus rather than remaining confined to the inner lining. As this tissue responds to hormonal changes during the menstrual cycle, it can cause inflammation, swelling, and irritation within the uterine muscle. Over time, this may lead to a uterus that becomes enlarged, thickened, and tender.
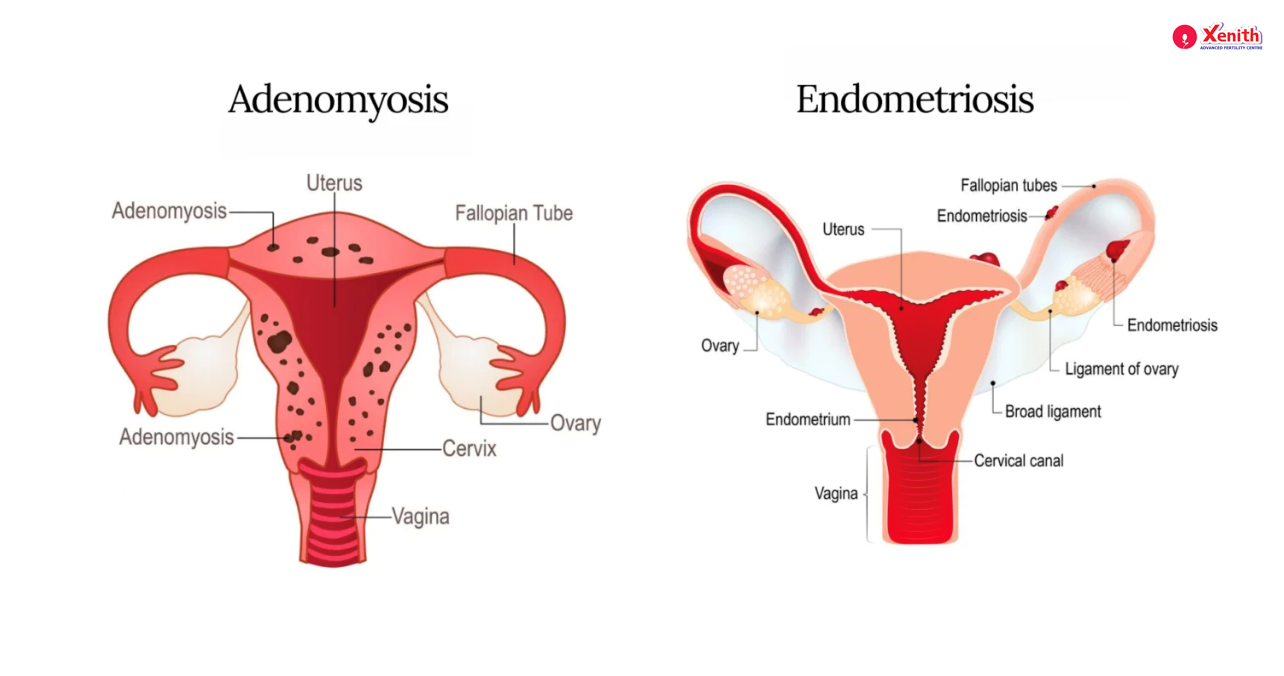
Patients sometimes ask me whether adenomyosis is the same as endometriosis. While the two conditions are related, they are not identical. In endometriosis, tissue similar to the uterine lining grows outside the uterus, often on the ovaries, fallopian tubes, pelvic lining, or nearby organs. In adenomyosis, the tissue remains within the uterus but grows into the muscular wall.
To make matters more complicated, many women may have both conditions at the same time. This overlap can contribute to diagnostic confusion and may explain why symptoms sometimes seem more severe or difficult to categorize.
Adenomyosis vs. Endometriosis: What’s the Difference?
One of the most common questions I receive from patients is how adenomyosis differs from
endometriosis. While they share certain symptoms, they affect the body in different ways.
Feature | Adenomyosis | Endometriosis |
Location of tissue growth | Within the muscular wall of the uterus | Outside the uterus on pelvic organs and tissues |
Typical age of onset | Often diagnosed in women in their 30s and 40s, though it can occur earlier | Frequently begins during reproductive years and may be diagnosed at younger ages |
Pain pattern | Heavy periods, severe cramps, pelvic pressure, uterine tenderness | Pelvic pain, painful periods, pain during intercourse, bowel or bladder symptoms |
Effect on uterus shape | May cause a diffusely enlarged or bulky uterus | Usually does not enlarge the uterus itself |
Diagnostic method | Primarily ultrasound and MRI findings | Imaging may help, but diagnosis can sometimes require surgical evaluation |
Typical fertility impact | May affect implantation and uterine environment in some women | Can affect ovarian function, fallopian tubes, pelvic anatomy, and fertility |
Although these conditions differ, they can coexist. This is one reason why a thorough fertility evaluation often involves looking for multiple possible contributors to symptoms and reproductive challenges.
Common Symptoms of Adenomyosis
Many women live with adenomyosis symptoms for years without realizing that what they’re experiencing isn’t simply a “normal” period. In my practice, I often see patients who have accepted significant discomfort as part of everyday life.
Common symptoms include:
- Heavy or prolonged menstrual bleeding (menorrhagia) that may interfere with daily activities.
- Severe menstrual cramps, often becoming more intense with age.
- Chronic pelvic pain that can occur even outside of menstruation.
- An enlarged or tender uterus, sometimes causing a feeling of pelvic heaviness or pressure.
- Pain during intercourse, which may affect quality of life and relationships.
One thing I always remind my patients is that severe pain and heavy bleeding should not be considered something you simply have to “put up with.” If your periods regularly disrupt your work, social life, or overall well-being, it’s worth seeking a proper evaluation.
How is Adenomyosis Diagnosed?
The diagnosis of adenomyosis has improved dramatically over the past decade. Historically, a definitive diagnosis could only be made by examining uterine tissue after hysterectomy. This meant many women were diagnosed only after surgery performed for other reasons.
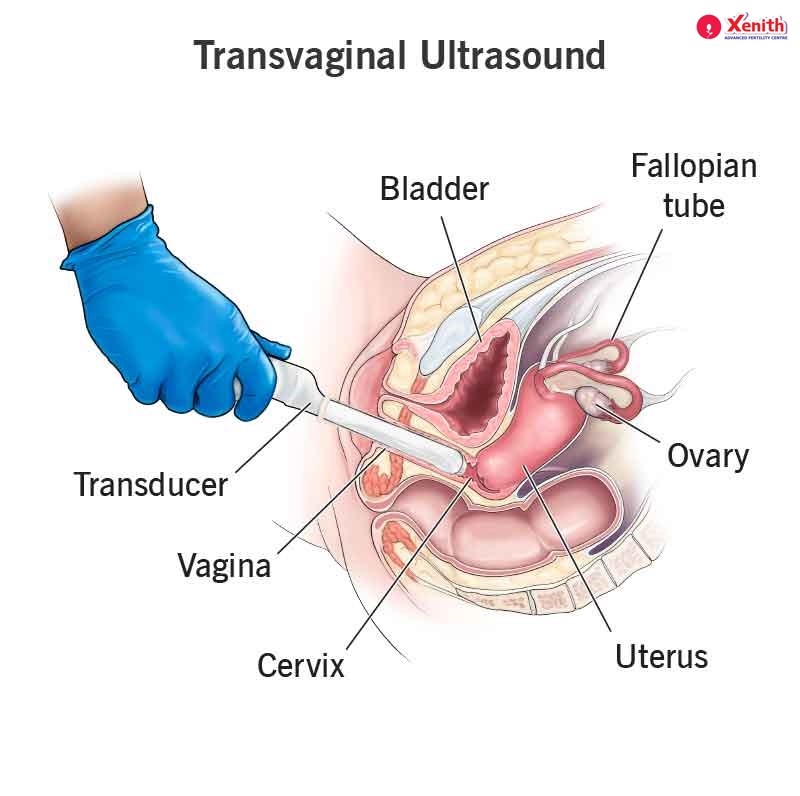
Today, advanced imaging techniques allow us to identify adenomyosis much earlier and without surgery in most cases. The first-line diagnostic tool is usually a transvaginal ultrasound. This test is widely available, non-invasive, and highly useful when performed by clinicians experienced in evaluating uterine conditions. On ultrasound, we may look for features such as a thickened uterine muscle layer, small cystic areas within the muscle, asymmetry of the uterine walls, or a generally enlarged appearance of the uterus. These findings can suggest adenomyosis, although no single ultrasound feature alone provides absolute certainty.
In cases where additional detail is needed, MRI can be particularly helpful. MRI offers a more detailed view of the uterine structure and may be used when ultrasound findings are unclear or when treatment planning requires further evaluation.
Modern imaging has significantly reduced the need for surgical confirmation, allowing many women to receive a confident diagnosis while preserving fertility and avoiding unnecessary procedures.
How Does Adenomyosis Affect Fertility and IVF Outcomes?
This is often the question patients worry about most after receiving a diagnosis. The relationship between adenomyosis and fertility is an area of active research, and the scientific evidence is more complex than many online sources suggest.
Several theories have been proposed to explain how adenomyosis might influence fertility. These include altered uterine contractility, changes in the implantation environment, and localized inflammation within the uterine muscle. Researchers believe these factors may potentially affect embryo implantation or early pregnancy development in some women.
However, it is important to present the evidence honestly. Some studies have reported reduced implantation rates, lower pregnancy rates, or increased miscarriage rates among women with adenomyosis. Other studies have found that these differences become less pronounced or disappear entirely when factors such as age, body mass index, and coexisting fertility conditions are carefully accounted for.
This is why I caution patients against viewing adenomyosis as a guaranteed barrier to pregnancy. Instead, I encourage them to think of it as one factor among many that a fertility specialist will evaluate when developing a treatment strategy. Many women with adenomyosis conceive naturally. Many others achieve successful pregnancies through IVF and other fertility treatments. The diagnosis is important, but it is not a prediction of failure.
Treatment Options for Adenomyosis
Treatment depends on several factors, including symptom severity, age, fertility goals, and the presence of other reproductive conditions.
For women primarily seeking symptom relief, hormonal therapies are often considered. Medications such as GnRH agonists or progestin-based treatments can help reduce pain, bleeding, and inflammation. In fertility treatment settings, these medications may also be used strategically before embryo transfer to optimize the uterine environment.
Surgical treatment is sometimes considered in select cases. However, surgery is generally approached cautiously when future fertility remains a priority. The specific role of surgery varies considerably depending on the individual patient’s circumstances.
For women pursuing IVF, treatment often focuses on improving the uterine environment before embryo transfer. In some cases, this may involve a longer down-regulation protocol or other adjustments tailored to the patient’s diagnosis.
One of the most important messages I share with patients is that there is no single universal protocol for adenomyosis. What works well for one patient may not be appropriate for another. Treatment decisions are individualized based on the complete clinical picture.
Can You Get Pregnant Naturally with Adenomyosis?
Yes. This is one of the most reassuring facts I can share with patients.
Adenomyosis does not automatically mean infertility, and many women with the condition conceive naturally. The likelihood of pregnancy depends on multiple factors, including the severity of adenomyosis, a woman’s age, ovarian reserve, and whether other fertility conditions are also present.
For example, coexisting endometriosis, fibroids, tubal disease, or male-factor infertility may have a greater impact on fertility than adenomyosis alone.
In some situations, fertility specialists may recommend pursuing IVF or other assisted reproductive technologies sooner rather than later. This is particularly true when age-related fertility decline is also a consideration. The decision is always individualized, taking into account both the diagnosis and the patient’s broader reproductive goals.
How Xenith Approaches Adenomyosis in Fertility Treatment
At Xenith, our approach begins with understanding the complete picture rather than focusing on a diagnosis in isolation.
When evaluating adenomyosis, we combine imaging findings with a detailed medical history, symptom assessment, menstrual patterns, fertility goals, and any coexisting reproductive conditions. This comprehensive approach helps us determine not only whether adenomyosis is present, but also how significant it may be within the context of a patient’s overall fertility journey.
For patients pursuing fertility treatment, we develop personalized strategies that account for uterine factors while considering age, ovarian reserve, embryo quality, and other relevant variables. Our philosophy aligns closely with the personalized infertility treatment approach that guides care throughout the clinic.
Over the years, I have worked with many women facing complex uterine conditions, including adenomyosis, endometriosis, fibroids, and combinations of these diagnoses. One lesson I’ve learned repeatedly is that fertility care works best when it is individualized rather than protocol-driven. Every patient’s story is different, and treatment should reflect that reality.
FAQs
Is adenomyosis the same as endometriosis?
No. Adenomyosis involves endometrial tissue growing within the muscular wall of the uterus, while endometriosis involves similar tissue growing outside the uterus.
Can adenomyosis be cured?
Treatment can effectively manage symptoms and improve quality of life, but there is no single universal cure that applies to all patients. Management depends on symptoms, age, and fertility goals.
Does adenomyosis always cause infertility?
No. Many women with adenomyosis conceive naturally and carry healthy pregnancies. The condition may influence fertility in some cases, but it does not automatically cause infertility.
What is the best age to seek treatment if I suspect adenomyosis?
If you experience persistent symptoms such as heavy bleeding, severe menstrual pain, or fertility concerns, it is advisable to seek evaluation regardless of age rather than waiting for symptoms to worsen.
Can adenomyosis come back after treatment?
Some symptoms can recur after certain treatments, particularly if the underlying hormonal influences remain active. Long-term management plans vary by individual.
Does adenomyosis affect IVF success rates?
Research findings are mixed. Some studies suggest reduced implantation or higher miscarriage rates, while others find little difference once other factors are considered. Your fertility specialist will assess adenomyosis as one part of your overall fertility profile.
You Don’t Have to Keep Living With Unanswered Symptoms
One of the most common things I hear from women diagnosed with adenomyosis is that they wish they had sought answers sooner. Symptoms that have been normalized for years such heavy bleeding, severe cramps, chronic pelvic pain, or fertility struggles deserve a proper medical conversation. If you suspect adenomyosis or have been experiencing symptoms that affect your quality of life, I encourage you not to dismiss them as something you simply have to endure.
At Xenith, we’re here to help you understand what’s happening and explore the most appropriate treatment options for your individual situation.
Book a consultation and pelvic ultrasound evaluation at our Wakad or Koregaon Park clinic. Together, we can take the next step toward clarity, symptom relief, and a fertility plan tailored to your needs.
📅 Ready to start or continue your IVF journey? |
• Book an in-clinic appointment at Wakad or Koregaon Park |
• Schedule a Video Consultation with Dr. Mamta Dighe |
• Call us: +91 91307 76776 | Email: info@xenithivf.com |
|